Archive for July, 2008
July 30, 2008
This could have been such a great article, had the question just been tweaked a little bit. (Therapy Watch: Diving In – How quickly should you open up in therapy?) Rather than “How quickly should you open up in therapy?” I think that “How quickly do you open up in therapy?” Or, since the article paneled all therapists…. “How quickly do your patients open up in therapy?”
I think that there are few “shoulds” in therapy (although I can think of a lot of should-nots!), but I am curious to know how long it takes others to settle in with a new therapist… I’m sure there are so many different variables (situation, diagnosis, type of therapist, previous treatment history, age, frequency of treatment, etc.), but how long does it take you to feel comfortable with a new T?
If I had to answer the question myself, my response would be, “Depends — how insightful is the therapist?”
If the therapist is going to wait for me to come out of my shell and tell her my story when I decide the time is right… it will probably never happen. Why bother? I need some indication of interest or insight or something. A couple of months back, my neurologist put two and two together (Wellbutrin + amenorrhea) and asked if I had any history of anorexia. And then if I had had an MRI because it could be hypothalamic amenorrhea. These questions of course lead to, “Well… ,” which leads to information that my therapist in college probably never even knew.
I’m not advocating a “don’t ask, don’t tell” policy… but it sure does help the “opening-up” process when you ask the right questions.
Technorati Tags: anorexia, bulimia, eating disorder, depression, treatment, therapist, eating disorder treatment, eating disorder recovery, mental health, mental illness, new therapist, ED therapist, recovery
Tags:Anorexia, bulimia, depression, eating disorder, eating disorder recovery, eating disorder treatment, ED therapist, ED treatment, mental health, mental illness, new therapist, recovery, therapy
Posted in eating disorder, Pop Psych, therapist | 3 Comments »
July 29, 2008
To build on yesterday’s post… I have quite a few “rules” that seem very logical to me. Not really eating disordered rules, like “no liquids with calories”… although some of those do still linger (at the height of my disorder, I could have probably written a book with all of my rules). No, these are different — we’ll just call them “Grey Logic.” Obviously they are influenced by recent events / arguments.
1. You must abide by “ED recovery etiquette” — By this I mean, no matter how crappy you are doing, when you go out with a friend that you know has an ED or whom you know from treatment, you better suck it up and act as normal as possible… because triggering a friend is not okay.
2. If I can’t get a salad for dinner, neither can you — And I can’t, because then it would be considered eating disordered. So order something else.
3. It’s not fair for you to skip breakfast and skimp on lunch, and then give me crap when dinner isn’t my largest meal of the day — While you were sleeping, I was enjoying the most important meal of the day (breakfast). All meals being equal, your skipping 1.5 of them doesn’t put you in a position to be criticizing my dinner.
4. Please please please don’t order the same thing as me at a restaurant — Because restaurants are challenging enough, and I don’t want to be comparing how much I ate to how much you ate.
5. Don’t eat my yogurt — I’m sure this is unique to me… but there are 100 kinds of yogurt in the world — why eat mine? I think it’s more the switch from a different yogurt to my yogurt that bothers me…
6. Things you can’t say: You’ve lost weight. You haven’t had an appetite lately. Wow grey, you’re always cold — you must have no metabolism. You’ve doubled your workout plan lately. You’re not eating ____ food anymore. Our friend has lost so much weight. Our friend needs to gain weight — she’s too thin.
,,, I could go on, but I’ll stop. feel free to add your own 🙂
Technorati Tags:
anorexia, bulimia, eating disorder, eating disorder treatment, mental health, mental illness, eating disorder recovery, eating disorder rules, logic, losing weight
Tags:Anorexia, bulimia, eating disorder, eating disorder recovery, eating disorder rules, logic, losing weight, mental health, mental illness, no appetite
Posted in Anorexia, eating disorder, Personal | 7 Comments »
July 29, 2008
To build on yesterday’s post… I have quite a few “rules” that seem very logical to me. Not really eating disordered rules, like “no liquids with calories”… although some of those do still linger (at the height of my disorder, I could have probably written a book with all of my rules). No, these are different — we’ll just call them “Grey Logic.” Obviously they are influenced by recent events / arguments.
1. You must abide by “ED recovery etiquette” — By this I mean, no matter how crappy you are doing, when you go out with a friend that you know has an ED or whom you know from treatment, you better suck it up and act as normal as possible… because triggering a friend is not okay.
2. If I can’t get a salad for dinner, neither can you — And I can’t, because then it would be considered eating disordered. So order something else.
3. It’s not fair for you to skip breakfast and skimp on lunch, and then give me crap when dinner isn’t my largest meal of the day — While you were sleeping, I was enjoying the most important meal of the day (breakfast). All meals being equal, your skipping 1.5 of them doesn’t put you in a position to be criticizing my dinner.
4. Please please please don’t order the same thing as me at a restaurant — Because restaurants are challenging enough, and I don’t want to be comparing how much I ate to how much you ate.
5. Don’t eat my yogurt — I’m sure this is unique to me… but there are 100 kinds of yogurt in the world — why eat mine? I think it’s more the switch from a different yogurt to my yogurt that bothers me…
6. Things you can’t say: You’ve lost weight. You haven’t had an appetite lately. Wow grey, you’re always cold — you must have no metabolism. You’ve doubled your workout plan lately. You’re not eating ____ food anymore. Our friend has lost so much weight. Our friend needs to gain weight — she’s too thin.
,,, I could go on, but I’ll stop. feel free to add your own 🙂
Technorati Tags:
anorexia, bulimia, eating disorder, eating disorder treatment, mental health, mental illness, eating disorder recovery, eating disorder rules, logic, losing weight
Tags:Anorexia, bulimia, eating disorder, eating disorder recovery, eating disorder rules, logic, losing weight, mental health, mental illness, no appetite
Posted in Anorexia, eating disorder, Personal | 7 Comments »
July 28, 2008
Half of Americans are dieting these days (not an official statistic) — and I can’t handle being around any of them. That rules out a lot of potential relationships! But really… I don’t handle being around dieting well. I don’t need anyone around me counting calories or skipping meals. Why? Because:
1. I’ve spent enough time in my life counting calories (and want those hours back!
2. It’s triggering
3. I feel guilty for eating more, weighing more, needing more, wanting more, thinking I deserve more, etc
4. Paranoia that I’m eating too much
5. I’m a little competitive
I’ve been extremely lucky to find very normal eaters for friends… relatively healthy eaters, but non-dieting friends. We get ice cream, go out for pizza, have snacks, etc. And this is all so so so helpful.
I visited family a couple of weekends ago, and my two younger sisters are dieting. I don’t think they have eating disorders (knocking on wood). One is out of college and the other is half-way through. Yes, I know that 1/3rd of women at Renfrew are now adults… but I’d like to think that they would have shown disordered behaviors by now were either of them prone to developing an ED.
My parents don’t discourage the dieting… actually I’d go so far as to say that they support it. You wouldn’t think this would be the case after having one daughter in and out of treatment facilities for most of high school… but I guess my parents never really did get involved with treatment. Anyway, when I told my mother that my boyfriend would be coming, she was excited to bake because “no one around here eats anymore.” Yes, this was going to be a problem…
The drive to my parent’s house was eight hours, and apparently my boyfriend does not like to stop for meals or snacks along the way. Notice that unless we were driving in the middle of the night (which we were not), this interferes with the “normal eating” model.
I realize that it’s probably normal for people to skip an occasional meal (I’ve talked about this before), but sometimes I feel like I should wear a sign: Warning: Do not approach if you do not eat 3 meals and a snack.
Technorati Tags:
eating disorder, anorexia, bulimia, mental health, mental illness, counting calories, recovery, skipping meals, eating disorder recovery, meal plan
Tags:Anorexia, bulimia, counting calories, Dieting, eating disorder, eating disorder recovory, meal plan, mental health, mental illness, recovery
Posted in eating disorder, Personal | 5 Comments »
July 20, 2008
While it may have just been a “thought experiment,” it was great to read this post from Laura Collins. As I mentioned in my Dr. Drew entry, I think that eating disorder recovery and long-term maintenance needs to be taken as seriously as other addictions. Using even once isn’t okay… so why is losing a pound?
I think that cutting corners signifies a change in mindset. It doesn’t matter if you’re still technically eating a normal amount of calories… if you’re not following your meal plan, you’re restricting. Sure, there are some behaviors that are just habitual… but for the most part, the behaviors are going to follow your thoughts. So, if you’ve been cruising along pretty well in recovery for awhile… and then start occasionally skipping little things… that is significant.
My question now is… is skipping a meal every once in awhile maybe normal? And if it is… does that make it okay for someone with an ED history to skip a meal on occasional? Or, are they never able to have that degree of flexibility because of their past and genetic predisposition?
I’ve been visiting family this past week. On the drive up here (9 hours), my boyfriend decided he wasn’t getting lunch — not hungry. I wasn’t terribly hungry and wans’t about to stop and eat by myself. By the 5th hour of the trip, though, I was ready to have a breakdown (I’m sure low blood sugar was no helping) over my boyfriend skipping lunch. He definitely doesn’t have an eating issue, but I still need the people around me to eat normally ALL the time.
Am I capable of just skipping an occasional meal — assuming that’s normal? I guess missing one meal isn’t a big deal. But what kind of parallel can you draw between than a drug/alcohol addiction? Will I feel the need to restrict again? Will I feel like it’s justifiable because other people skip meals?
The lines between healthy and unhealthy, normal and eating disordered, are all blurred. Is there less of a grey area if you’ve struggled with an eating disorder in the past? Could someone else’s habits be fine for them, but disordered for me?
Tags:Anorexia, bulimia, Dr. Drew, eating disorder, eating disorder treatment, healthy relationship with food, Laura Collins, mental health, mental illness, skipping meals, treatment
Posted in Anorexia, eating disorder, Websites | 4 Comments »
July 20, 2008
While it may have just been a “thought experiment,” it was great to read this post from Laura Collins. As I mentioned in my Dr. Drew entry, I think that eating disorder recovery and long-term maintenance needs to be taken as seriously as other addictions. Using even once isn’t okay… so why is losing a pound?
I think that cutting corners signifies a change in mindset. It doesn’t matter if you’re still technically eating a normal amount of calories… if you’re not following your meal plan, you’re restricting. Sure, there are some behaviors that are just habitual… but for the most part, the behaviors are going to follow your thoughts. So, if you’ve been cruising along pretty well in recovery for awhile… and then start occasionally skipping little things… that is significant.
My question now is… is skipping a meal every once in awhile maybe normal? And if it is… does that make it okay for someone with an ED history to skip a meal on occasional? Or, are they never able to have that degree of flexibility because of their past and genetic predisposition?
I’ve been visiting family this past week. On the drive up here (9 hours), my boyfriend decided he wasn’t getting lunch — not hungry. I wasn’t terribly hungry and wans’t about to stop and eat by myself. By the 5th hour of the trip, though, I was ready to have a breakdown (I’m sure low blood sugar was no helping) over my boyfriend skipping lunch. He definitely doesn’t have an eating issue, but I still need the people around me to eat normally ALL the time.
Am I capable of just skipping an occasional meal — assuming that’s normal? I guess missing one meal isn’t a big deal. But what kind of parallel can you draw between than a drug/alcohol addiction? Will I feel the need to restrict again? Will I feel like it’s justifiable because other people skip meals?
The lines between healthy and unhealthy, normal and eating disordered, are all blurred. Is there less of a grey area if you’ve struggled with an eating disorder in the past? Could someone else’s habits be fine for them, but disordered for me?
Tags:Anorexia, bulimia, Dr. Drew, eating disorder, eating disorder treatment, healthy relationship with food, Laura Collins, mental health, mental illness, skipping meals, treatment
Posted in Anorexia, eating disorder, Websites | 4 Comments »
July 10, 2008
Have you ever been told that “food is your medicine?” According to a study at UCLA, it quite literally can be. It’s no secret that healthy eating is important, but did you know that:
- Salmon, walnuts, and kiwi protect against depression, mood disorders, and schizophrenia?
- You’re at a greater risk for ADD, depression, bipolar, and even schizophrenia if you have an omega-3 dietary deficiency?
- Omega-3s actually increase verbal intelligence, learning, and memory? (someone should have told me that years ago — maybe I would have done better in organic chemistry…)
- Your diet can effect the mental health of your grandchildren?
- Junk food decreases cognitive function? (and we’re not just talking sugar-comas)
You hear about the physical benefits of omega-3s, folic acid, etc. all the time… but not as often about their relationship with mental health (and illness).
These findings also demonstrate the self-perpetuating nature of eating disorders… eating less can just contribute to depression, which often results in more disordered eating… so, you have the original contributing factors + low body weight (resulting in increased anxiety/depression, OCD, etc.) + malnutrition (and all the cognitive negatives). That’s a lot working against you!
This news also has a lot of potential for “alternative medicine” treatment. I think that psych meds are very over-prescribed… and they come with so many side effects that eating fish sounds like a much better option (or at least a good adjunctive treatment).
Technorati Tags: anorexia, bulimia, eating disorder, mental illness, mental health, alternative medicine, diet and memory, UCLA, food and the brain, diet and mental illness, depression
Tags:alternative medicine, Anorexia, bulimia, depression, diet and memory, diet and mental illness, eating disorder, food and the brain, mental health, mental illness, UCLA
Posted in eating disorder, Health, mental health, nutrition, Pop Psych, research | 7 Comments »
July 9, 2008
The relationship between ghrelin, amenorrhea, and eating disorders has been examined time and time again. The consensus seems to be that persistent amenorrhea is likely attributed to disordered eating rather than low body weight. I’ll admit that I am particularly interested in this subject because I do have hypothalamic amenorrhea. This finding is interesting for a few reasons:
1. Return of menses is often a benchmark of physical recovery. Goal weights are subject upon your menstrual cycle… if you’re still not getting your period, then you still don’t weigh enough.
2. If you really are at a healthy weight and still don’t get your period, then it just needs to be “jump-started.” I was told this for years without the professional questioning my current ED behavior.
3. I’ve known several eating disordered women who lost their period well within (or above) the healthy weight range. This study clearly shows how possible that is.
4. If you read the study, those with hypothalamic amenorrhea actually consumed MORE calories than those with normal menses. Granted they score higher on the EAT, but still… I wish someone would explain how this is possible — aside from basing it purely on purging behavior. I just have this cartoon image in my head of my body trying to communicate that it disapproves of food rituals 🙂
Now, I realize the adaptive value of this condition… from an evolutionary perspective, not enough expendable energy = not a good time to get pregnant. If you put a modern twist on this, nature seems to be saying: Hey, you’re still not taking care of yourself — no way should you be influencing a kid! You know… kinda limiting the anorexic/bulimic population…
Technorati Tags: eating disorder, anorexia, bulimia, disordered eating, amenorrhea, ghrelin, physical recovery, treatment, mental health, mental illness, healthy weight, Eating Attitudes Test
Tags:amenorrhea, Anorexia, bulimia, disordered eating, Eating Attitudes Test, eating disorder, ghrelin, healthy weight, mental health, mental illness, physical recovery, treatment
Posted in depression, Websites | 2 Comments »
July 7, 2008
I have just been waiting to write about this article all day!
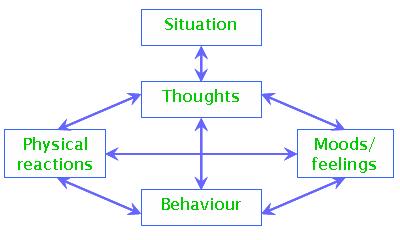
Cognitive Behavioral Therapy
“The [UK] government has earmarked £173m to increase the number of cognitive behavioural therapists in the NHS.””Professor Mick Cooper, an expert in counselling at the University of Strathclyde, told the conference at the University of East Anglia that although he welcomed the increased funding for psychological therapies, the focus on CBT was not logical.
He and three colleagues from the UK and US issued a statement saying there had been more studies on CBT, but that did not necessarily mean it was more effective than other types of therapy.
“It is scientifically irresponsible to continue to imply and act as though CBTs are more effective, as has been done in justifying the expenditure of £173m to train CBT therapists throughout England.
“Such claims harm the public by restricting patient choice and discourage some psychologically distressed people from seeking treatment,” he said.”
- This argument reminds me of my Dr. Drew Westen grad seminar days… Everyone is using CBT because it’s the easiest to research, has the most funding, etc. etc. Can’t say that I disagree — there is definitely too much hype about CBT. However, I don’t think that most professionals follow CBT guidelines even 75% of the time — it’s just not practical! Dr. Cooper has a great explanation of this:
“What is more, where researchers have allegiances to one particular approach, the control ‘therapies’ that are developed to test these approaches against often bear little relationship to those approaches as actually practiced in the field, and cannot really be considered therapeutic at all (Wampold, 2001, p.104) (Shapiro and Shapiro (1982) refer to these approaches as ‘straw men’). In the Foa et al. (1991) study of PTSD in women who had been raped, for instance, therapists in the ‘supportive counselling’ condition were instructed that, if their clients started to talk about their assault, they should redirect them to focus on current daily problems! “
Every therapist is going to respond similarly to some extent… maybe one is going to focus on though restructuring more than childhood, but you’re still going to have that consoling feeling. I think that whatever this common feeling is makes up the healing component of therapy… which is why the best predictor of treatment outcome is therapeutic alliance. This common set of elements that spans the different types of therapies has been termed the ‘Dodo bird’ verdict. I’ll have to write a post on that later…
Anyway, it’s nice to see someone arguing against CBT for a change! The world (and psych field) could use a little more psychoanalysis 🙂
Technorati Tags:
eating disorders, anorexia, bulimia, CBT, talk therapy, psychotherapy, therapist, psychology, psychoanalysis, NHS, psych research, treatment, mental illness, mental health, Dodo bird
Tags:Anorexia, anxiety, bulimia, CBT, depression, Dodo bird, eating disorders, mental health, mental illness, NHS, psych research, psychoanalysis, psychology, psychotherapy, ptsd, talk therapy, therapist, treatment
Posted in Article, Pop Psych, therapy | 7 Comments »
July 7, 2008
I have just been waiting to write about this article all day!
Cognitive Behavioral Therapy
“The [UK] government has earmarked £173m to increase the number of cognitive behavioural therapists in the NHS.””Professor Mick Cooper, an expert in counselling at the University of Strathclyde, told the conference at the University of East Anglia that although he welcomed the increased funding for psychological therapies, the focus on CBT was not logical.
He and three colleagues from the UK and US issued a statement saying there had been more studies on CBT, but that did not necessarily mean it was more effective than other types of therapy.
“It is scientifically irresponsible to continue to imply and act as though CBTs are more effective, as has been done in justifying the expenditure of £173m to train CBT therapists throughout England.
“Such claims harm the public by restricting patient choice and discourage some psychologically distressed people from seeking treatment,” he said.”
- This argument reminds me of my Dr. Drew Westen grad seminar days… Everyone is using CBT because it’s the easiest to research, has the most funding, etc. etc. Can’t say that I disagree — there is definitely too much hype about CBT. However, I don’t think that most professionals follow CBT guidelines even 75% of the time — it’s just not practical! Dr. Cooper has a great explanation of this:
“What is more, where researchers have allegiances to one particular approach, the control ‘therapies’ that are developed to test these approaches against often bear little relationship to those approaches as actually practiced in the field, and cannot really be considered therapeutic at all (Wampold, 2001, p.104) (Shapiro and Shapiro (1982) refer to these approaches as ‘straw men’). In the Foa et al. (1991) study of PTSD in women who had been raped, for instance, therapists in the ‘supportive counselling’ condition were instructed that, if their clients started to talk about their assault, they should redirect them to focus on current daily problems! “
Every therapist is going to respond similarly to some extent… maybe one is going to focus on though restructuring more than childhood, but you’re still going to have that consoling feeling. I think that whatever this common feeling is makes up the healing component of therapy… which is why the best predictor of treatment outcome is therapeutic alliance. This common set of elements that spans the different types of therapies has been termed the ‘Dodo bird’ verdict. I’ll have to write a post on that later…
Anyway, it’s nice to see someone arguing against CBT for a change! The world (and psych field) could use a little more psychoanalysis 🙂
Technorati Tags:
eating disorders, anorexia, bulimia, CBT, talk therapy, psychotherapy, therapist, psychology, psychoanalysis, NHS, psych research, treatment, mental illness, mental health, Dodo bird
Tags:Anorexia, anxiety, bulimia, CBT, depression, Dodo bird, eating disorders, mental health, mental illness, NHS, psych research, psychoanalysis, psychology, psychotherapy, ptsd, talk therapy, therapist, treatment
Posted in Article, Pop Psych, therapy | 7 Comments »


